
Coming too you live from the 2014 Paediatric Anaesthetic Congress of Southern Africa (PACSA 2014), being held at the Vineyard Hotel Conference Centre. Kudos for these quick notes transcribed and kindly provided by my dear friend and colleague Dr Matthew Gibbs
PACSA 2014

Opening Address – Prof Wim de Villiers: Dean
10 C’s of research
Clinical: the only need is the patients need.
Critical thinking
Collaboration
Courage to break out of old furrows
Constructive structures for research
Cooperative partners (day care for researchers etc)
Consent: detailed
Clinical research: who has the ownership of the research question? Interests in companies?
Chronophage: young researchers being asked to do extra stuff that eats into your time!
Caring mentor
Prof Mariana Kruger: PhD. Tygerberg. Paediatric oncologist
Off label and unregistered drug use in paediatrics- our ethical responsibility
Purpose is to benefit the patient. Not illegal. Just not on insert.
Therapeutic decision-making- best available evidence.
Paeds TBH- INH the most common off label use.
Call to collaborate and publish evidence. Ensure dialogue. Actively participate in dialogue with MCC. Drive registration process (in US anyone can register a drug).
Advocacy. Suitable registered preparations when available. Use extemporaneous drugs only if absolutely necessary. Create awareness regarding extemporaneously prepared drugs. It seems that some anti TB drugs are made with chloroform. Share information with other SADC countries. MONITOR adverse drug reactions.
Evidence base? Two comparative studies. Gold standard– double. Double blind randomized control trials. Rare diseases- problematic. Rely in expert opinion. Act in best interest of patients. Document! And publish results.
Physician responsible for he decision about the drug and he dose, and advocate and promote paediatric drug studies. Rare diseases: crossover, N of. 1. Randomized withdrawal trial. Maybe a journal of a NEGATIVE studies! Prevent repeating studies. Health care founders should not use labeling status as the sole criteria for reimbursement decisions.
Dr Karmen Kemp, Red Cross War Memorial Children’s Hospital
Does the paediatric epidural still have a leg to stand on?
Benefits: decreased stress, adrenaline, cortisol levels, better wound healing, faster return of gut healing, decreased ventilator days, decreased happy talk stay, more effective analgesia. Risk: transient complication 2.5:10000, longer term 1:30000. Risks acceptably low. Risk benefit is favorable. Medico legal environment in South Africa is catching up faster to first world standard than the medical care! This means fewer epidural insertions and worse skills. Reasonable care vs highest measure of professional skill. What about other alternative analgesia? IV paracetamol. Clonidine, dexmedetomidine, gabapentin. Wound infusion catheters, US guided nerve blocks and field blocks.
Evidence: adults: continuous wound infiltration not inferior to epidurals. No Paeds studies. Seems to be similar benefit. Epidural vs continuous TAP blocks: again comparative. What about safety of TAP blocks. Upper limit 0.3%. Cather kinking or leaking. Very minor. Safe alternatives to epidural.
What about nursing? Desperately need skilled sisters. Nursing levels are too low. Commonly need to admit to ICU for epidural care! High staff turnover, agency personnel, policy driven. Standard operating procedures. Guidelines, and policies available for nursing for epidurals in children in the UK. Collaborative approach is recommended. Need to work together in training and supporting our nursing staff. Epidural service is possible, current levels of staffing or support inadequate for an epidural service. Field blocks are safe and easy esp with US. This is resulting in fewer epidurals, along with skills and safety. Therefore starting to change to worsening risks and therefore risk benefit will change.
So what can we do? Better policies and guidelines. Continue education and skills training. Clear documentation. Novel strapping techniques. US use for space determination. Beware doing less than 100 epidurals per year. Drug errors… Epidural paracetamol!
Red Cross: 60-80 per year. On average I will see 5.8 epidurals per 6 month training over 4 years. 2-3 paediatric epidurals actually performed! Not the ‘highest measure of clinical skill’!
Save the epidural! Therefore 24h support, develop SOP, follow up, system of documentation. Continued training and teaching. Must go through nursing structures for their approval and buy in. Is it worth saving the paediatric epidural? YES! Must maintain skills as an option at least. Audit risk profile of epidural service in South African context.
Dr Jonathan de Lima Sydney. Children’s hospital at Westmead.
Chronic regional pain syndrome in children
Department of pain medicine and palliative care.
Four areas: acute pain management, chronic and complex pain, cancer pain and palliative care, and N2O procedural sedation.
The anaesthetists perspective on chronic regional pain syndrome. These are the worst cases of this condition.
Case study: 14y 82kg. Jarred knee- recurrent pain and swelling. Ketamine infusion, Celestine sciatic injections. Massive range of drugs! Poly pharmacy. Leg immobile. Pain at rest 9/10. Depressed. Vasomotor changes. Will not allow any touching of leg. Social isolation, weight gain, school disruption. Now what?
Epidural under GA. Bupivicaine and clonidine. Aggressive treatment and intense physio and desensitization. D14 discharged ambulant and pain free. Still discharged baclofen, Gapabentin etc. but weaned regardless of pain scores!
First desprciotion in American civil war 1864 Silas Mitchell. Now CRPS with or without nerve injury. Typical story older women, Colles fracture. Then develops chronic pain. Upper limb, 5-7th decade, women more than men.
What about children? 20 kids it Westmead. 90% girls! lower limb in 85%, 80% reported trauma. Big delay in referral. Pts of MRIs and XRs. Physio and psych interventions. 50% admission, lots of readmission and relapse. 2 weeks on average admission. Clinical presentation distinguished from adults, by occasional extreme sensory disturbance, tremor and dystopias less common, parental enmeshment, need for behavioral management, children regarded as high achievers, and compliant. high rate of family and marital discord.
2nd case. Admitted under physicians. 13 y old. Upper limb. CRPS. Joint hyper mobility syndrome. Multisystem phenotype, benign. But full blown: anxiety disorders and panic attacks. “Constitutionally determined brain-body interactions underlie this psychosomatic vulnerability”. Joint hyper mobility may represent a sub-type of anxiety disorders. this child roomed with first case: saw how amazing the block was, and insisted on block. Have to get into parents minds that real treatment is physio. Problem is brain has blue screen of death: need to control alt delete. That’s what the blocks does. So under GA, peformed block, in theatre EUA and physio. Catheter inserted. Desensitization programme, scale back on opioids. Aggressive therapy again. Monitored by looking at handwriting and art work.
What about pathophysiology? An update on CRPS by Warner. Multiple mechanisms. Abnormal inflammatory process, genetic predisposition, CNS change in neurons. fMRI shows changes. Some objective changes found. Ockham’s razor: the more assumptions you need to make for a theory to be true, the less likely it is that the theory is true. One single unifying theory? What might it look like? ResolvinsnRvE1 in Nature Medicine 2010. Inflammatory processes have amplifying mechanisms. What about resolving inflammation? Washing away, passive resolution? In fact, it is an active process. Resolvins and Protectins.
Therapeutic options: Blocks are done in a minority. Good physio is CRITICAL! www.aci.health.nsw. gov.au/chronic-pain/painbytes. In Sydney, they no longer use pharma ,TNF antibodies or spinal cord stim, mirror techniques.
Final case. 9 y old. Bilateral CRPS, screaming in bed. Severe behavioral abnormalities. Despite dense surgical block with epidural, she woke up screaming in pain. Severe parental discord. Still better in 10days- physio with ear plug! Warning: patient developed superficial cellulitis over epidural site D5 infusion: very scary.
Out on a limb: adolescent ward, unknown pathophysiology, no evidence for treatment efficacy, poly pharmacy, prolonged neuraxial infusions. Inefficient resource allocation. ?best model of care. Critical: maximum physio time with patient whilst epidural is in. Tunneled catheters: 2cm below skin.
Dr Tracy Kilborn. Red Cross
Imaging of mediastinal masses in children
Clear guidelines, radiation is an issue, lifetime cumulative dose. Genetic, sex and age susceptibility. Shared responsibility.
Doses: CXR 0.03mSv. AXR 30 CXRs. Ct0T chest 100-180XRs.1 death from cancer from radiation per 1200 CT scans!
Excellent views but comes at a cost.
MRI: sedation GA, hostile environment. Length of scans, hostile environment. US operator dependent, surgeons don’t like/understand images.
Www.imagegently.com
Ok, let’s start with a CXR. Difficult to perform. Technically problems. Normal shouldering of trachea, slight deviation away to the right from the aortic arch. Tracheal buckling normal with poor inspiration. Need good expiratory films. Rotation? Can’t comment on lucency or tracheal masses if rotated.
Lateral XR helps a lot.
Para tracheal stripe not more than 4-5mm. Hilar regions should be concave not convex. Para tracheal stripe and hilar regions are middle mediastinum. Posterior mediastinum: look at aortic shadow.
Anterior mediastinum: thymus, Germ cell tumours, lymph nodes. From lateral: thymus hugs the sternum always. Over the age of 5 if you see a thymus, it is abnormal. Is it abnormal? US good modality. Moves around like a bath sponge, homogenous. If heterogenous, then abnormal.
Middle mediastinum: vascular: double arch, aberrant subclavian. LAD. Tracheal lesions, Cysts. How do we identify structures? Know anatomy: oesophagus and trachea. Left and right main pulmonary arteries and aortic arch. Look at lateral. Also look at splaying of carina. Shouldn’t look like a cowboy on his horse.
TB often presents as posterior mediastinal mass.
Remember: evaluate technique of exam.
Know anatomy: AP And lateral
Consider alternatives to CT.
CUMULATIVE radiation doses is a shared responsibility.
Tracheal resections.
Dr Jacques Janson
50% of pediatric thoracic surgery is TB gland enucleations.
Tracheal stenosis: short segment complete tracheal rings (<30%). Primary resection owns anastomosis. Difficult sharing airway. Longer sections? More than 30%. Pericardial patch (poor outcome). More popular: slide tracheoplasty. Leaves potential for growth. Can extend to bronchus. One options is to share airway: but technically challenging. CPB much simpler. Prolonged intubation, granulomata, malacia. Mortality still 20-25%.
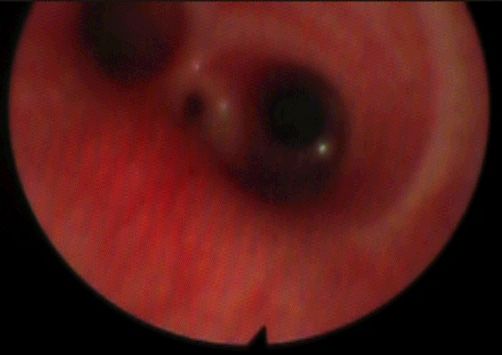
Post intubation tracheal stenosis. Avoid tracheostomy! CXR and CT. Bronchi soy and serial dilation. Want to know how far the TS is from the VCs, how long it is! and how far to carina.
Vascular compression: can be from Innominate artery, pulmonary arteries and aorta. Sx with Ba swallow, CT chest. Echo important: 10% have other cardiac effects. Bronchoscopy for dynamic compression.
Complete rings: Double aortic arches. Different forms thereof.
Incomplete rings: e.g. Pulmonary artery slings. Aberrant Innominate artery.
Dr Rik de Decker, Red Cross Cardiology
‘Echoes of Brilliance’
Intellectual history of echo.
“Throughout the brilliance of any images, resound with the echoes of the past”.
Bats and ultrasound.
Sonar. Speed cameras.
Echolocation to echocardiography.







{kind=link}